
Today I decided to answer a simple but very important question. Is it possible to distalize molars on the lower jaw?
Very often we see today clinicians attempt to push the lower molars distally to create space in the dental arch.
But how far can the molars be pushed back? How stable will the result be? And if this manoeuvre is at all possible?
Let’s find the answers…

Maxillary distalization
First, let’s look at the distalization on the maxilla. This has been done for many decades for Class II correction since the times of Edward Angle. Current evidence tells us that this method is rather effective and stable. Given that there is enough bone behind the second molars we can get on average 2-4 mm of distalization with a relapse of only about 0.1 mm per year [1,2].
Mandibular distalization
But what about the mandibular distalization? The orthodontists of the past never dared doing it. It seems that only the implementation of temporary anchorage devices in the early 2000s got us into this controversial topic.
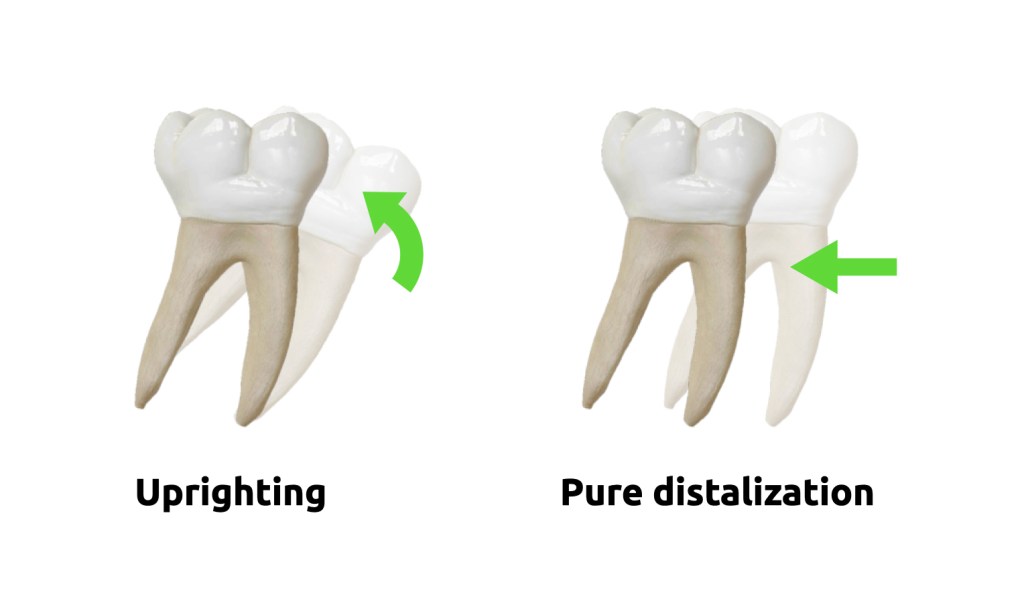
Before we look at the numbers, I want to highlight an important distinction. Molars can be pushed back in two different ways. The first one is called uprighting. It is when only the molar crown tips back while the root apexes stay put. The second one is called pure distalization. It is when the force is applied through the center of resistance and we reach a bodily movement of both the crown and the roots. In reality it is often a combination of uprighting and pure distalization.
In their study of mandibular distalization published in the AJO-DO in 2004 the authors used miniplates as an anchor [3]. They distalized the lower molars in 15 adult patients.
They found that the average amount of distalization of the mandibular first molars was 3.5 mm at the crown level and 1.8 mm at the root level. In other words, they were able to get only 1.8 mm of pure distalization. Furthermore, they found that an annual relapse was 0.3 mm at both the crown and root apex levels. As a result, we may suggest that pure distalization on the mandible relapses to 100% in 6 years.
We also have to consider that in their study the authors used a very effective method of anchorage. Miniplates ensure a very rigid anchorage and provide 3 times the amount of mandibular distalization compared to miniscrews [4]. But it seems that even such a great anchorage method can not defy the rules of anatomy. We know from classic studies that arch lengths decrease with age in all of our patients [5,6]. Moreover, some studies clearly suggest that this happens mostly due to mesial molar movement rather than distal incisor movement. With more pronounced changes on the mandible [7].
What do I think?
I think that, if needed, mandibular molar uprighting works great. However it’s important to understand that we can’t upright already uprighted teeth. The lower molars are considered to be uprighted if they are angulated 2 degrees mesially. This is according to Lawrence Andrews’ classic study of 120 naturally perfect dentitions.
I also think that mandibular molar distalization is a losing battle and shouldn’t be attempted. We will probably continue witnessing beautifully photographed attempts of this unscientific endeavour on social media but we have to remind ourselves (and our patients) that this is done primarily out of ignorance.
References
1. Shoaib AM, Park JH, Bayome M, Abbas NH, Alfaifi M, Kook YA. Treatment stability after total maxillary arch distalization with modified C-palatal plates in adults. Am J Orthod Dentofacial Orthop. 2019 Dec;156(6):832-839. doi: 10.1016/j.ajodo.2019.01.021. PMID: 31784017.
2. Mohamed RN, Basha S, Al-Thomali Y. Maxillary molar distalization with miniscrew-supported appliances in Class II malocclusion: A systematic review. Angle Orthod. 2018 Jul;88(4):494-502. doi: 10.2319/091717-624.1. Epub 2018 Apr 17. PMID: 29664335; PMCID: PMC8191939.
3. Sugawara J, Daimaruya T, Umemori M, Nagasaka H, Takahashi I, Kawamura H, Mitani H. Distal movement of mandibular molars in adult patients with the skeletal anchorage system. Am J Orthod Dentofacial Orthop. 2004 Feb;125(2):130-8. doi: 10.1016/j.ajodo.2003.02.003. PMID: 14765050.
4. Yeon BM, Lee NK, Park JH, Kim JM, Kim SH, Kook YA. Comparison of treatment effects after total mandibular arch distalization with miniscrews vs ramal plates in patients with Class III malocclusion. Am J Orthod Dentofacial Orthop. 2022 Apr;161(4):529-536. doi: 10.1016/j.ajodo.2020.09.040. Epub 2021 Dec 23. PMID: 34953658.
5. Little RM, Wallen TR, Riedel RA. Stability and relapse of mandibular anterior alignment-first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod. 1981 Oct;80(4):349-65. doi: 10.1016/0002-9416(81)90171-8. PMID: 6945805.
6. Paquette DE, Beattie JR, Johnston LE Jr. A long-term comparison of nonextraction and premolar extraction edgewise therapy in “borderline” Class II patients. Am J Orthod Dentofacial Orthop. 1992 Jul;102(1):1-14. doi: 10.1016/0889-5406(92)70009-Y. PMID: 1626523.
7. Boley JC, Mark JA, Sachdeva RC, Buschang PH. Long-term stability of Class I premolar extraction treatment. Am J Orthod Dentofacial Orthop. 2003 Sep;124(3):277-87. doi: 10.1016/s0889-5406(03)00448-7. PMID: 12970661.
