
As William Proffit laconically put in 1990:
“The indication for surgical-orthodontic treatment is that a skeletal or detoalveolar deformity is so severe that the magnitude of the problem lies outside the envelope of possible correction by orthodontics alone.”1
However, what lies outside and what lies within is usually a subjective decision. And whereas I have little doubts that an experienced orthodontist or maxfac surgeon won’t have any difficulty making this decision, I think it is great to have clear diagnostic guidelines to help less experienced colleagues to opt between surgical vs camouflage treatment choice in borderline class III cases.

Personally, I just assess the magnitude of skeletal discrepancy and the degree of dentoalveolar compensation on the radiographic images. That is usually enough for me to understand whether I am dealing with a surgical case, but I have never had exact cephalometric numbers in my mind.
Although recently I came across a nice study published by the group from Iran in Progress in Orthodontics journal in 2018:
The authors aimed to:
“delineate diagnostic measures in borderline class III cases for choosing proper treatment.”
They included retrospective data from 36 camouflage patients and 29 surgical patients. Three board-certified orthodontists approved the treatment course and results of the selected cases.
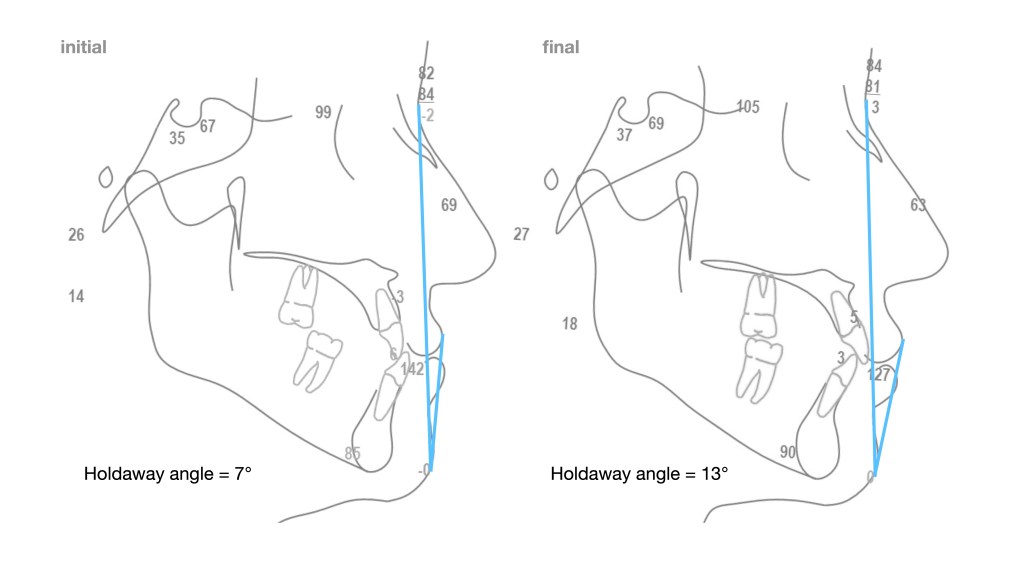
The authors decided to base their assessment on two cephalometric parameters – Holdaway angle and Wits appraisal.
They concluded:
“Borderline class III malocclusion patients who have a Holdaway angle greater than 10.3° would be treated successfully by camouflage alone, while surgery should be the treatment of choice in borderline class III malocclusion patients with a Holdaway angle of less than 10.3°. This study also showed that Wits appraisal greater than −5.8 mm would be effectively corrected by camouflage and less than −5.8 mm must be treated by surgery.”
I think it is great to have these numbers by which younger clinicians can double-check their treatment choices.
Below is my recently finished case which seems to be in agreement with the figures provided by the authors.
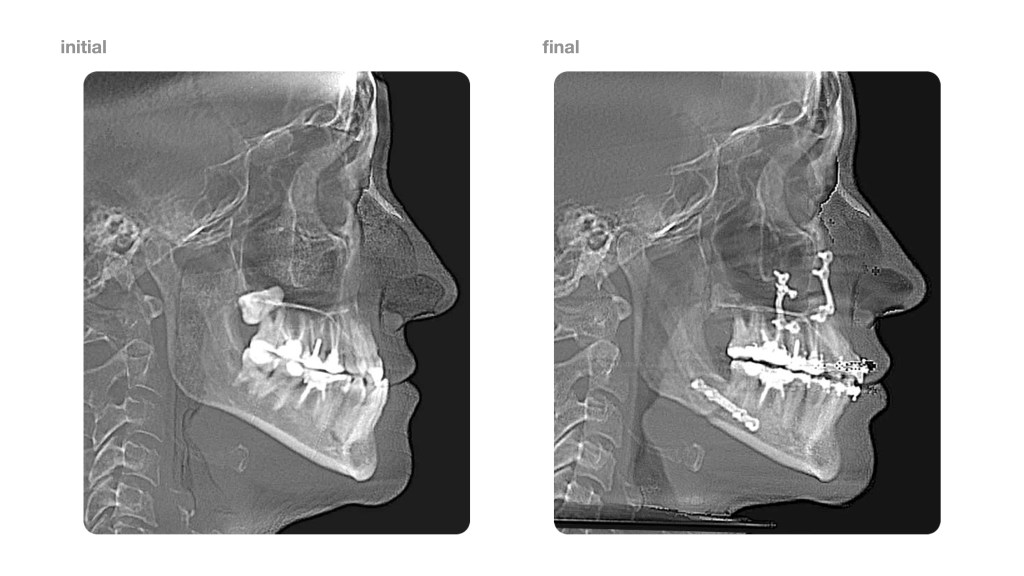

Surgery is performed by Dr. Andrey Senyuk at Face Smile Center in Moscow, Russia.
1. Who needs surgical-orthodontic treatment? W R Proffit, R P White Jr; Int J Adult Orthod Orthognath Surg, 1990;5(2):81-9
